A Bundibugyo Ebola outbreak with no approved vaccine, active armed conflict, and deepening community mistrust has crossed into a new phase of operational failure. Events in the first days of June underscore how far containment has slipped.
The Outbreak Has Already Spread Across More Than 20 Health Zones
The World Health Organization declared a Public Health Emergency of International Concern on May 16, 2026 — one day after health authorities identified the virus. But the pathogen had been circulating undetected for months before that identification, giving it time to move across Ituri, North Kivu, and South Kivu provinces. By early June 2026, health workers had recorded more than 900 suspected cases and 220 suspected deaths. Confirmed figures stood at more than 340 cases and at least 60 deaths spanning more than 20 health zones. The gap between suspected and confirmed counts is itself a signal: conflict-driven access restrictions mean the true scale of the outbreak is likely undercounted. The following metrics reflect the publicly reported situation as of early June.
Four Compounding Barriers Are Blocking Every Standard Response Tool
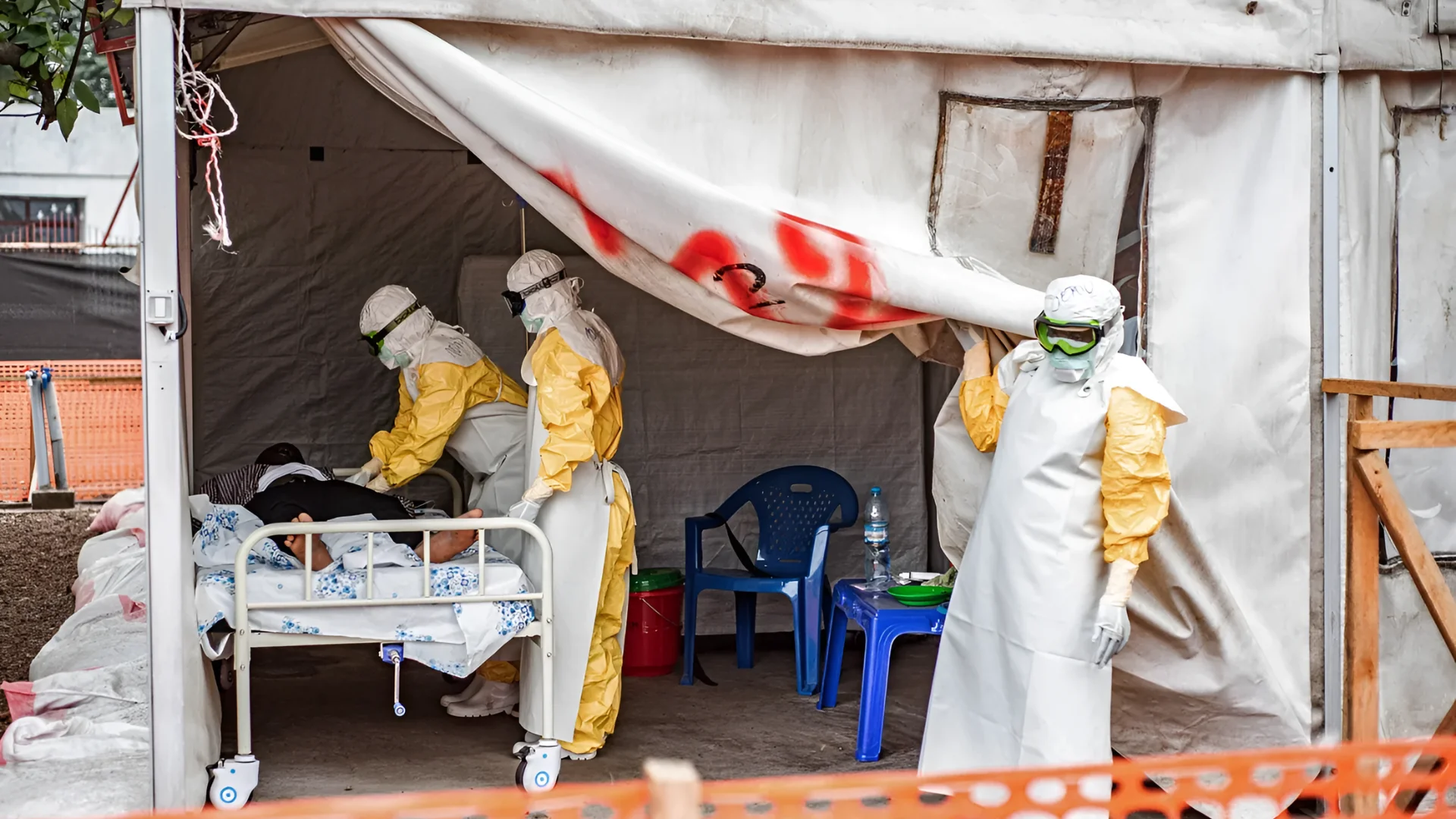
What makes this outbreak operationally different from prior Ebola responses is not any single obstacle but the way four distinct barriers reinforce each other. The absence of an approved vaccine or therapeutic for the Bundibugyo strain means containment depends entirely on isolation, contact tracing, and safe burial — the three functions most directly damaged by the other three barriers. Armed conflict across Ituri, North Kivu, and South Kivu, where rebel militias including the ADF, CODECO, and M23 operate, limits humanitarian access and pushes displaced populations into crowded camps where transmission risk rises. Community mistrust, which WHO Director-General Tedros Adhanom Ghebreyesus called a "serious barrier," has driven patients to flee isolation facilities and led residents to attack response teams. On June 1, a specialized safe-and-dignified burial team in the rebel-controlled town of Katana was attacked and forced to abandon a coffin; community members then handled the highly infectious body directly. That kind of contact with an Ebola-positive body during the hemorrhagic stage carries a high transmission probability and represents a potential amplification event, not merely a protocol failure. Eleven patients escaped isolation facilities in the epicenter province of Ituri, with similar reports from Bunia. For a detailed breakdown of why standard containment tools won't work in this environment, see our earlier analysis. The chart below scores each barrier by operational severity, using an ordinal editorial assessment derived from the described conditions in reporting from Bloomberg, Reuters, and the NYT.
A Timeline of How This Outbreak Escalated From Silent Spread to PHEIC
Understanding the pace of escalation matters for gauging what comes next. The virus circulated for months before it was identified, meaning the detection gap itself built a structural deficit into the response. The PHEIC declaration on May 16 gave international responders formal authorization to coordinate and deploy resources, but it arrived after a long period of silent spread. The containment breaches of early June — the Katana burial attack and the patient escapes in Ituri — represent a further deterioration, not a stable holding pattern. Uganda's border closure with the DRC adds an economic pressure layer, disrupting the cross-border trade that many communities depend on and potentially deepening the mistrust that is already obstructing the response. For background on what is driving this outbreak at a structural level, see our earlier reported piece. The timeline below maps the five documented milestones from silent circulation to the June 2026 operational breaches.
The outbreak's trajectory — from silent spread to PHEIC to documented containment breach inside three weeks of public identification — reflects how much ground the virus covered before response operations could be fully established. With no approved vaccine or specific treatment for the Bundibugyo strain, and with the primary response tools of isolation and safe burial now demonstrably compromised in key epicenter areas, the operational picture entering June 2026 is one of deepening constraint rather than stabilization.

Alpha-Gal Syndrome: What a Tick Bite Does to Your Diet
Alpha-gal syndrome is a delayed food allergy caused by tick bites that sensitizes the immune system to a sugar molecule found in mammalian meat. Cases are surging in the Midwest and Northeast, with new state-level reporting mandates and federal labeling legislation underway.

ACOG Breaks from CDC on Maternal Vaccines in 2026
American College of Obstetricians and Gynecologists releases its own maternal vaccine schedule backing influenza, COVID-19, Tdap, and RSV shots, defying CDC rollbacks and countering RFK Jr.-era misinformation.

Ebola Bundibugyo Outbreak DRC: 676 Cases, No Vaccine
As of mid-June 2026, a rare Bundibugyo Ebola outbreak in DRC's Ituri Province has killed 138 people, spread to Uganda, and reached packed displacement camps with no licensed medical countermeasures available.

Daraxonrasib Nearly Doubles Pancreatic Cancer Survival
Trial results presented at ASCO 2026 show daraxonrasib nearly doubled median survival in advanced pancreatic cancer — a look at the data, the mechanism, and what remains unproven.
Comments (0)
Please sign in to join the discussion.
No comments yet.
Be the first to share your perspective on this topic.